By: Richard Caro | Posted: January 18, 2021 | Updated: April 5, 2023
Photo by Paper Textures
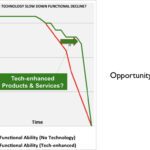
The opportunities seem bigger than ever, but the products we hoped for have by and large not emerged as yet.
Here are some gerontech products we wish existed.
The Context
We started Tech-enhanced Life back in 2014 with the idea that there were big opportunities for new products (incorporating various types of technology) — to significantly postpone the time at which frailty and functional disability would get in the way of “living life”.
How do I feel at the end of 2020?
Well, I am pleased to say there seem some glimmers of promise (see “Technology for Older Adults: Notable from 2020“). However, overall I would say that the opportunities seem bigger than ever, but that the products we hoped for have not emerged as yet.
The reasons why this field, known as gerontechnology or agetech, has thus far fallen short of our expectations for exciting new products are complex, and not the focus of this article.
But there are a handful of product concepts which in my opinion seem extremely promising, but which do not yet exist as commercially available products — although the technology to enable them already largely exists.
This article is to briefly describe them.
Gerontech Products That Could Make a Big Impact
We picked a handful of gerontech product ideas for this article, with the idea that these are products we think could make a big difference to the lives of many, but which in our opinion do not exist today in a form accessible to “most people”.
The ideas (described in more detail further down the page) are:
- Gait or Balance Monitor + Predictive Score + Intervention;
- Cognition Monitor + History Over Time (+ Intervention?);
- Driving Ability Tester;
- Affinity Group Tools (especially virtual).
Why These Gerontechnology Ideas?
Of course, there are lots and lots of ideas for new products, and we see many of them.
Often they cluster into rather predictable categories — like fall alerts and medication management solutions. For this article, I wanted to focus on ideas that for whatever reason do NOT seem to be on the list of “things lots of people are working on”.
My other criteria was that they would be products that would “really move the needle” — in terms of impact on older adults themselves, or their families.
Some Caveats
This is an opinion piece. Others will likely have different opinions. I wanted to mention a few things that seemed relevant before diving into the ideas.
- The ideas ARE heavily influenced by the club meetings of our Longevity Explorers, in which we often discuss unmet needs and sometimes brainstorm ideas. (I have facilitated literally hundreds of these explorer club meetings over the last 5 years). These ideas do NOT arise from any of the explorations we have done with companies — the findings of which are confidential.
- These ideas are just that: ideas. They are based on deep immersion in the worlds of technology and aging, but have not been validated by us in formal studies of the sort one would do prior to deciding to commercialize them.
- There are other promising ideas too. This is not meant to be an exhaustive list.
- If you are thinking “so and so already thought of that”, you are likely right. This is not an effort to lay claim to these ideas. Just to socialize them.
- If you are thinking “that already exists”, that is great news. Feel free to tell us about it in the comments. Just check if whatever you have in mind really does the things we describe, and that it is actually something you can buy today.
- We do not have plans to commercialize any of these ideas ourselves. We would be delighted to see companies pick them up, and would be happy to collaborate with anyone who was interested in doing so.
- There are various research projects underway, and some startups that are focused on some of these ideas. We are not currently working with any of them (Dec. 2020), nor have we in the past, but we are hoping they will be successful.
- Yes, we realize there are significant issues related to regulation and “who pays”. We don’t mean to gloss over these, but they are for another article.
The Gerontech Innovation We Are Hoping For
There are some key themes that underpin these ideas, and which we believe are extremely important to older adults (the target customers), but under appreciated by the community of gerontech and agetech innovators.
Broadly speaking, these themes are about:
- Wellness vs sickness (this is a widely discussed topic in the circles of those interested in changing the current US healthcare system);
- The importance of autonomy as we grow older. Autonomy is something much valued, but which is typically an early casualty of any encounter with the aging services industry;
- Loneliness. It’s exciting to see this being much discussed recently, but we think the right solutions have yet to emerge.
Gait or Balance Monitor + Predictive Score + Intervention
It’s a truism to talk of falls being a big problem for people as they age. And there are many, many initiatives designed to address the “problem of falls“. (See our “Topic Hub”: Avoid the Perils of Falling for an overview of the issues and current solutions).
There are various “alerts” that “call for help” after you have fallen. And lots of fall risk reduction interventions (like exercise classes) designed to help reduce fall risk. And we think these are all useful and important.
BUT, alerting after you fall is less good than avoiding the fall in the first place. And balance exercises are only good if people do them, and human nature being what it is, they tend not to do things that are “good for them” (like eating broccoli) unless there is something that triggers them to focus on the issue.
We think a very powerful approach would combine several pieces that would together monitor fall risk over time, and offer appropriate interventions as needed. The ideal time for using this would be long before a person becomes at high risk for a fall. Think of it as a prophylactic.
We know of several startups with promising looking products in this space, but none has yet “emerged”. If and when that changes, we will update this.
Piece 1: Fall Risk Score
The first thing we want is a way to measure fall risk.
It does not need to be perfect, or absolute, although those would be good attributes. But it needs to measure and track a proxy for fall risk over time. And tell you something about where you stand compared to some metric of “goodness or badness”.
And when we say “fall risk” it can be some type of proxy for that, such as a metric derived from gait, or from balance.
And here are some critical features.
- The fall risk score needs to be given to you, as the older adult (ie you are in charge, not “the system”) — with educational tools so you know what it means.
- And ideally this would all happen at home, and not require a trip to see some type of healthcare person.
- And it would be up to the older adult to decide who was allowed to see the risk score, and what they would do about it.
- And it would track changes over time. Because often it would be changes over time that would trigger a desire to “do something” rather than an absolute number.
- And the risk score would need some peer-reviewed validation.
- In an actual product, maybe “fall risk” is the wrong terminology, and we would choose a more aspirational and positive term.
While clinicians have metrics of fall risk today, to our knowledge none of them has yet been turned into a service that meets all the criteria above and is widely commercially available. But we think they could be, relatively easily.
Piece 2: Intervention
There needs to be something you can do to improve your “fall risk” score, once you start to get worried about it.
The good news is that physiotherapists have some defined approaches to exercises for reducing fall risk, and so these interventions already exist. What is missing is connecting the fall risk score, with the features above, to the intervention.
We think there needs to be some out-of-the-box thinking that connects the fall risk to some defined coaching and or exercise services. This should go beyond “see your physiotherapist”.
There are good examples in the emerging digital health space of this type of coupling of monitoring and intervention (look for examples in the areas of diabetes management and weight loss).
Cognition Monitor + History Over Time (+ Intervention?)
It’s not news that Alzheimers and other forms of dementia are all too common, and big economic and clinical societal challenges. And for older adults facing the realities of growing older, the concern that something could happen to your mind is “a big deal”. (See our “Topic Hub”: Brain, Memory, Dementia Tech for background on this topic).
Of course, one can wait until one has dementia, and hope someone has come up with a “cure” by then. But for the more proactive, a preferred approach would be to try and “avoid it” — or reduce the risk of it happening to you.
There are two problems, which is where we see the opportunity for a new innovation.
Piece 1: Cognition Monitor
While not everyone wants something like this, there is a significant fraction of our explorer community who are interested in the idea of a “device” that could measure their level of cognition, and then track it over time.
And, if there was a proven intervention that could slow the decline of cognition, then the number of people interested in this would be much bigger.
An important aspect of this concept is that it would start to be used long before any cognitive decline manifested itself. In other words, it is a bit like an “engine warning light”. It doesn’t replace the visit to the doctor. It helps you remain “well” longer.
This “cognition monitor” would satisfy some rather similar criteria to the fall risk monitor above. We note that clinicians today have some tools that let them measure aspects of cognition (they use these to help diagnose dementia, for example). These do not satisfy all the criteria below, but we think it would not be hard to take existing techniques and adapt them.
Here are some critical features.
- It does not need to be perfect, or absolute, although those would be good attributes. But it needs to measure and track a proxy for cognition or dementia risk over time. And tell you something about where you stand compared to some metric of “goodness or badness”.
- The cognition score needs to be given to you, as the older adult (ie you are in charge, not “the system”) — with educational tools so you know what it means. It might need to involve a family member as well, or even instead, if there is signficant cognitive impairment.
- And ideally this would all happen at home, and not require a trip to see some type of healthcare person.
- And it would be up to the older adult to decide who was allowed to see the cognition score, and what they would do about it (perhaps with pre-agreed involvement of a family member at certain score levels?).
- And it would track changes over time. Because often it would be changes over time that would trigger a desire to “do something” rather than an absolute number.
- And the score would need some peer-reviewed validation.
- Especially important: the score would need to cover all the relevant aspects of cognition. It should not be limited to just one aspect (eg memory) if there are other aspects of cognition that matter for measuring dementia and cognition impairment.
- In an actual product, maybe “cognition score” is the wrong terminology. This would need thought.
Piece 2: The Intervention
First, the facts about whether there are interventions that can reduce dementia risk or slow down decline of cognition, and what they are, are hard to come by. The lay press is full of competing opinions. And many older adults are unclear.
So, some clear and credible education would be an important part of this “solution”.
Second, we believe that some of the interventions, like diet and exercise, would be more widely adopted if coupled with a metric that showed where one stood on the “cognition” ladder, and whether or not it was declining (and how fast).
As with the fall risk intervention above, we think the ideal product/solution would go far beyond saying “visit your physician”. There would ideally be some type of connected service to help decide what sort of intervention you needed, and ideally some type of motivational reinforcement, such as is common in the emerging field of digital therapeutics.
Driving Ability Tester
Several years ago, the Longevity Explorers held a series of brainstorming sessions built around questions like these.
- How do I know it’s time to stop driving?
- Who decides? Who should decide?
Some interesting things emerged from those brainstorming sessions. [See “When to Stop Driving: Who Decides, & How?” for details of these discussions.]
- Contrary to what many people think, in most states of the USA the DMV (Dept. of Motor Vehicles) does NOT measure the ability of people to drive when they renew their driver’s license — even for people at ages of 90+. Renewing the driver’s license requires a test of vision (in some states), and of the rules of the road after a certain age, but not of overall ability to drive (there is no driving test).
- The question of “who should decide it’s time to stop driving” is quite controversial.
Brainstorming a Solution
The Longevity Explorers brainstormed a “driving ability tester” solution, that had the following characteristics.
[There was some divergence between people who felt this solution should exist at the DMV for when you renewed your license, and those who wanted it at home.]
- It does not need to be perfect, or absolute, although those would be good attributes. But it needs to measure and track a proxy for “ability to drive safely” over time. And tell you something about where you stand compared to some metric of “goodness or badness”.
- The driving ability score needs to be given to you, as the older adult (ie you are in charge, not “the insurance company”) — with educational tools so you know what it means.
- And ideally this would all happen at home or in your car, and not require a trip to see some type of “evaluator”. Although some explorers felt this tool should exist at the DMV and be a requirement for getting your license renewed.
- And it would be up to the older adult to decide who was allowed to see the driving ability score from “their Ability Tester”, and what they would do about it.
- And it would track changes over time. Because often it would be changes over time that would trigger a desire to “do something” rather than an absolute number.
- And the score would need some peer-reviewed validation.
- Especially important: the score would need to cover multiple relevant aspects of driving ability. It should not be limited to just one aspect (eg road rules), because other factors are also important — like peripheral vision; ability to turn one’s head; speed of reaction; night vision adaptation times; and likely much more.
As with the prior ideas, this would be even better if coupled with some type of intervention to help improve your driving ability.
Affinity Group Tools (especially virtual).
Social isolation and Loneliness are important problems, and have received quite a bit of attention in the media in the last year or two. You can see various explorations we have conducted relating to this topic at our “Topic Hub”: Social isolation and Loneliness.
One of the big learnings for us as we have explored this topic has been that the people who need help with this issue are often NOT very outgoing or gregarious, and are often unenthusiastic about parties and one-on-ones with strangers. If you think about it, this makes sense. After all, outgoing social types are likely to be able to create their own social outreach initiatives if they wish.
Despite this, we notice that most of the initiatives we see that are targeted at “helping” with issues of social isolation and loneliness involve either “parties” (ie social gatherings to chat with others), or manufactured opportunities to interact one-on-one with strangers — with whom you might well have little in common.
While there is nothing wrong with these approaches, and they might work very well in some situations, we keep hearing about a different idea, and keep hoping to see it implemented in a way that is ideally suited to older adults “aging at home”. But so far we have not.
Here is the idea: Affinity Groups.
The core idea is that almost everyone is interested in “something”. And that getting together with a group of people, who have a strong interest in the same “something” as you do, is likely to be quite interesting to all involved.
And for those who are not naturally gregarious, think how much easier it is to engage in a discussion about that topic you spent years of your life being enthusiastic about, rather than struggling to find some topic to discuss with a stranger with no overlapping life experience or interests.
We call this an “affinity group”.
There have always been groups like this. Think book clubs, or sports fan clubs, or model train enthusiasts, or garden clubs, for example. And Meetup.org is a great example of a platform for affinity groups. And senior living communities often have lots of “clubs” that are really types of affinity groups.
The issues that arise, however, are:
- it’s sometimes hard or inconvenient to travel to wherever the affinity group is;
- maybe there is no affinity group for your interest within your geography;
- if you think of yourself as “older”, do you feel welcome?
So, what we envision is some type of hybrid face-to-face / virtual affinity group platform. With powerful tools for discovering “others like you”, and the ability to attend virtually if need be from your house, if you are restricted by circumstances from travelling. And a solution to helping older adults feel welcome.
Another key point: the affinity group needs to involve actual interaction with your fellow enthusiasts. Putting on “lectures” does not really meet our goals with respect to social isolation and loneliness.
Segregated?
So, should this platform be “segregated” (ie for older adults, not for “everyone”)?
We are not sure what the right answer here is. On the one hand, we are quite strongly of the belief that older adults in the USA would benefit from less age segregation rather than more. And there is no obvious reason why an affinity group should have age restrictions. After all, if you get together to discuss gardening or model trains, why is age a key issue?
On the other hand, we have noticed that when Meetup comes up in discussions among our explorers, a handful are already enthusiastic users of Meetup — while some others seem to have the opinion that “it is not for me”.
Bottom line re age segregation: we don’t have the answer, but are inclined against it.
Other Ideas
Of course, there are lots of other good ideas. We have some, and probably you do too. This is by no means an exhaustive list.
If you have ideas you want to share with the world, we think of this website as a platform where people with interesting ideas can share them. If you are interested, you can see more about how to collaborate and/or share your ideas with the world here.
Learn More. Engage With Us.
- If you are interested in any of these ideas, a good place to start would be to browse the relevant topic hubs (links above in the article), to see what else we have done relating to that topic.
- If you have some ideas on which you would like to collaborate, contact us and let us know.
- Want to learn when we publish more like this? Join our Newsletter.
*Disclosure: The research and opinions in this article are those of the author, and may or may not reflect the official views of Tech-enhanced Life.
If you use the links on this website when you buy products we write about, we may earn commissions from qualifying purchases as an Amazon Associate or other affiliate program participant. This does not affect the price you pay. We use the (modest) income to help fund our research.
In some cases, when we evaluate products and services, we ask the vendor to loan us the products we review (so we don’t need to buy them). Beyond the above, Tech-enhanced Life has no financial interest in any products or services discussed here, and this article is not sponsored by the vendor or any third party. See How we Fund our Work.